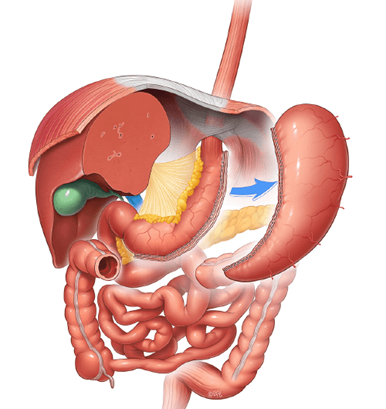
Sleeve Gastrectomy
A Sleeve gastrectomy (SG), also called sleeve or vertical gastrectomy, is a bariatric operation that removes approximately 75% of the stomach to leave a narrow gastric tube which restricts food intake. Both gastric emptying and intestinal transit are markedly increased after SG because the intra-gastric pressure increases upon ingestion of foods, which in turn increases the tension of the gastric wall.
The SG typically results in 25% to 35% body weight loss (50 to 70% excess weight loss) from baseline and most of the weight loss occurs in the first 6 months. The substantial weight loss may lead to dramatic improvement, and even complete remission of many of the obesity-related co-morbidities, including type 2 diabetes. Laparoscopic SG is rapidly becoming one of the most performed bariatric surgeries and sits in the intermediate position between the other two commonly performed bariatric procedures, laparoscopic adjustable gastric banding, and laparoscopic gastric bypass, in terms of surgical risk, weight loss and resolution of obesity-related illness. Although long-term data regarding the durability of the SG is regarded as inadequate, publications reporting intermediate follow up are favorable.
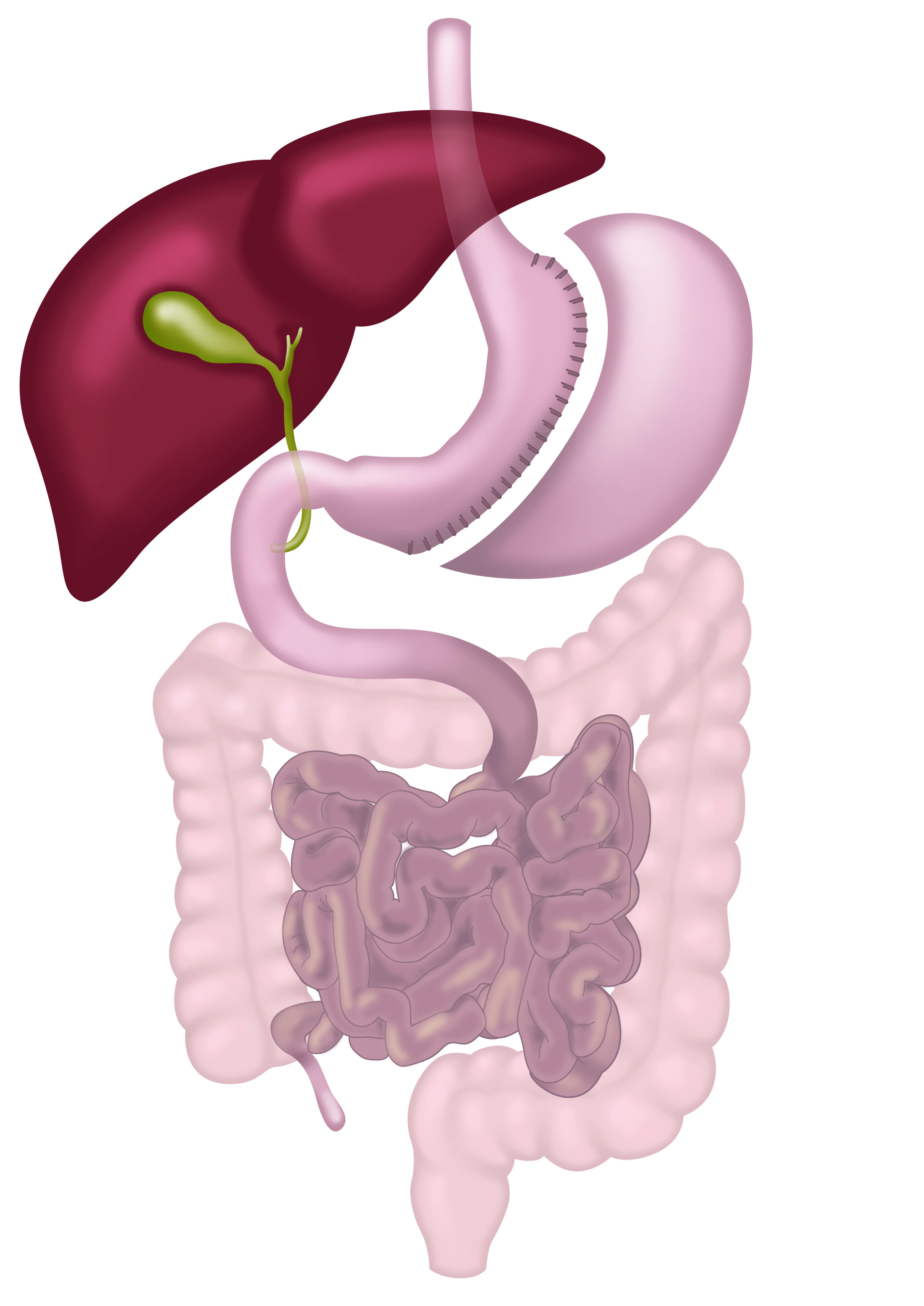
Sleeve gastrectomy
There are some advantages of the SG over the gastric bypass. SG is simpler and safer. It results in less vitamin and micro-nutrient deficiencies than the gastric bypass procedure. Other important advantages of the SG compared over gastric bypass are the lack of dumping syndrome and the avoidance of the risk of gastric cancer that arises from the excluded remnant stomach (though it is very low).
The main disadvantage of SG is that this procedure carries a 1-2% risk of leakage due to the long staple line of the gastric tube. Sleeve leaks are notorious for being more difficult to manage than gastric bypass leaks because of the high pressure in the gastric sleeve. Another drawback of the SG is the development of acid reflux symptoms. The incidence of reflux varies from 11 to 33% and requires prolonged use of medications, and sometimes even revision surgery.
Sleeve gastrectomy is recommended in patients with obesity class II or more (BMI ≥ 35 kg/m2)(1). For superobese patients (BMI ≥ 50 kg/m2), a two-step approach (in which the SG is the first part) may be advised to mitigate surgical risks.